Ceribell delivers clinically meaningful diagnostic information in the acute care setting
As your front-line STAT and 24-hour continuous EEG solution, Ceribell allows you to prioritize your time and use of conventional EEGs for the right patients
Time to EEG Matters
Even a two-hour delay in time to EEG can reduce response to first-line treatment by half.1 The longer the duration of seizure, the higher the mortality.2 Unlike stroke or cardiac arrest, most hospitals lack protocols to rapidly diagnose non-convulsive status epilepticus.
Treatment Response Rate1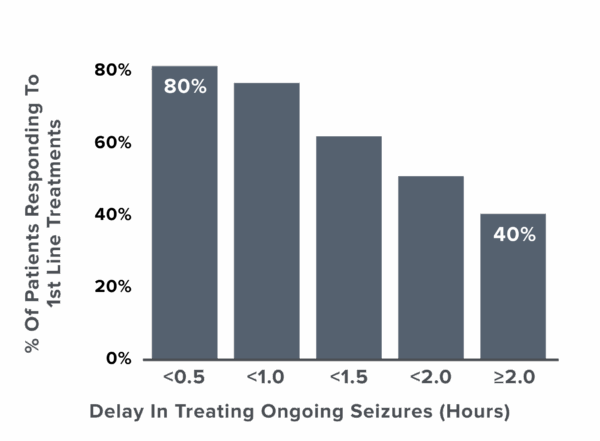
Time in Seizure is Associated with Increase in Mortality2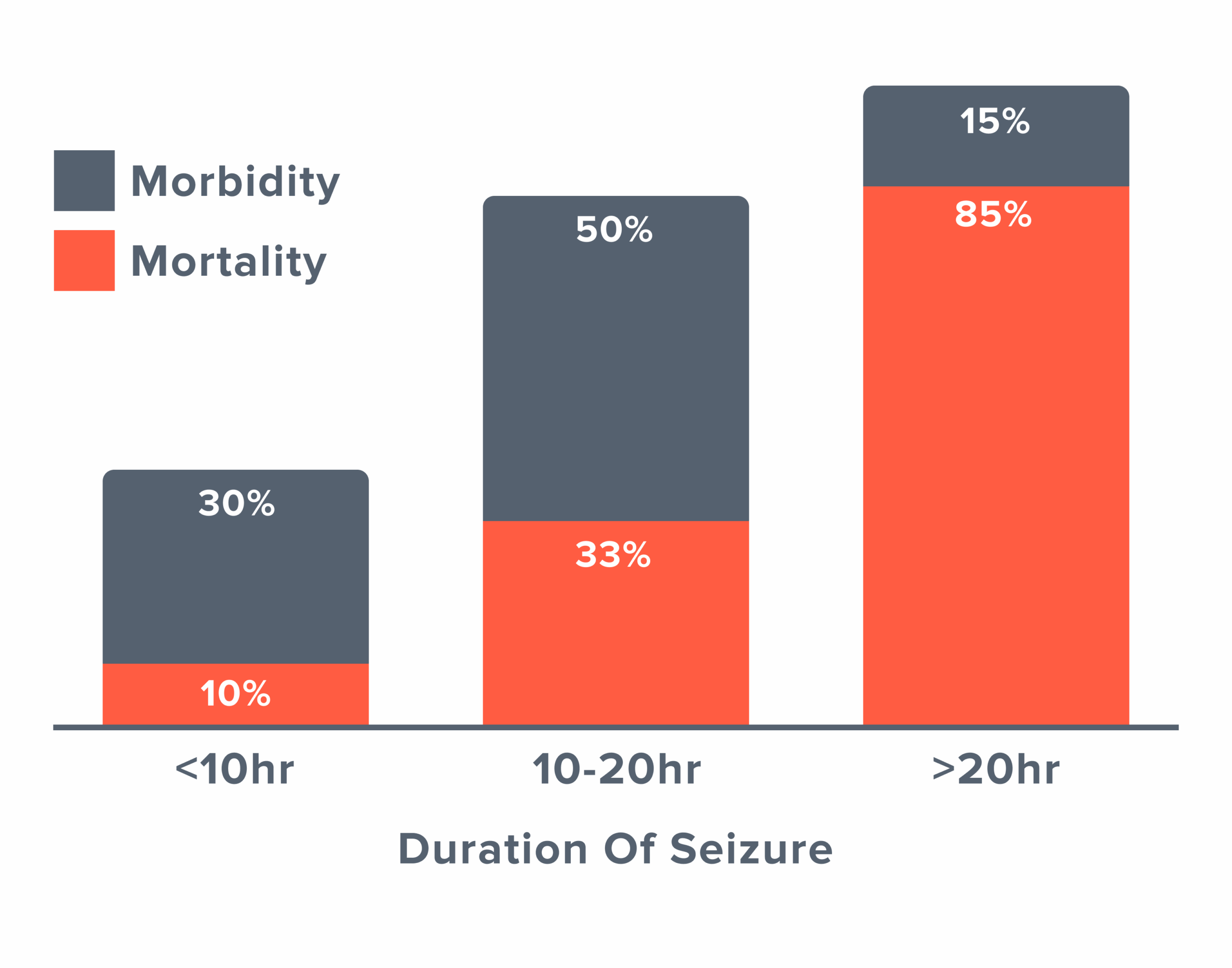
Guidelines Recommend Timely EEG to Detect and Manage Seizures

“Continuous EEG monitoring should be initiated within 1 h of SE onset if ongoing seizures are suspected.”

“Recommend promptly performing and interpreting EEG for the diagnosis of seizures in patients who do not follow commands after ROSC.”
Conventional EEG: Not Designed for Critical Care
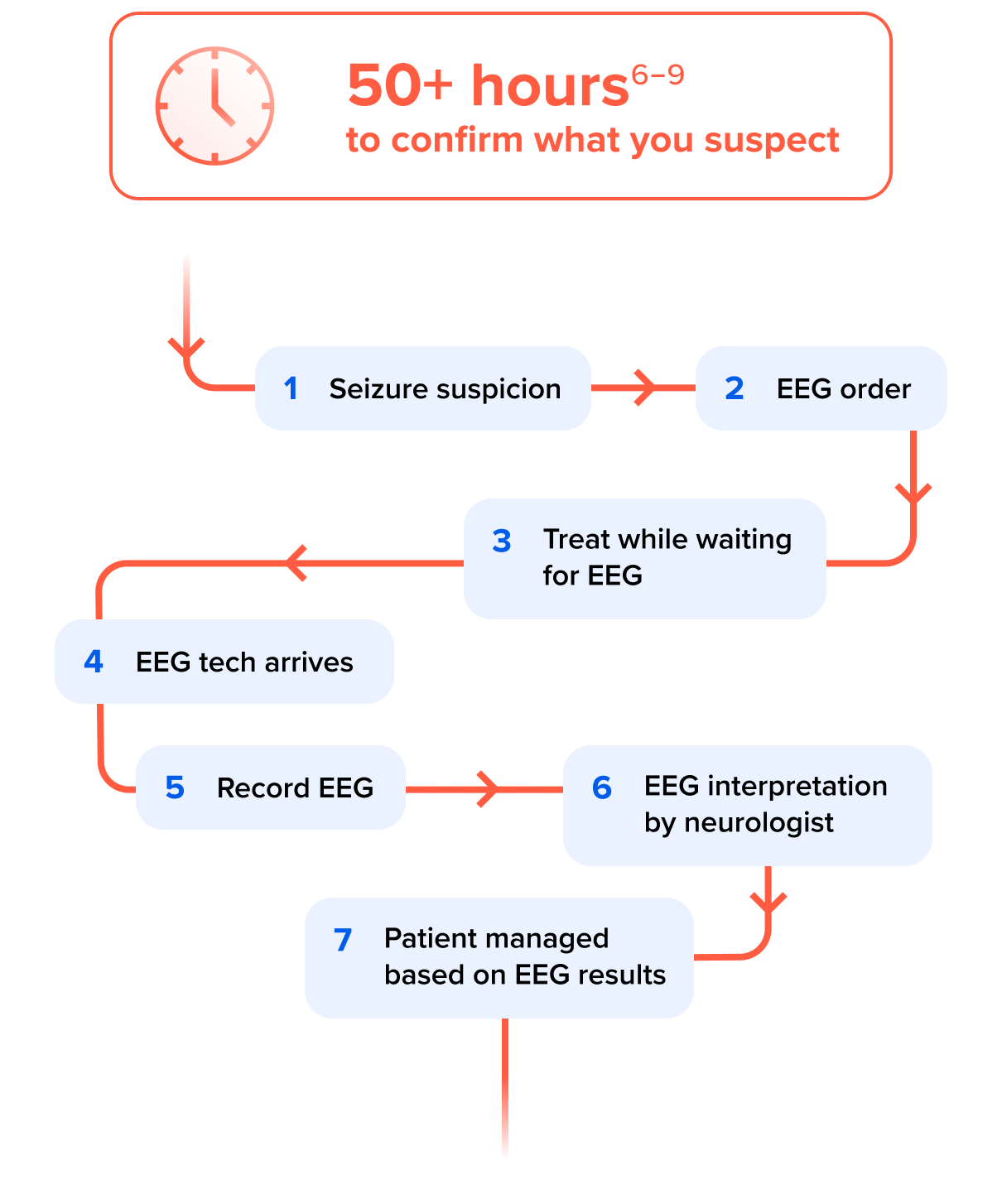
It can take hours, or even days, to administer and interpret a conventional EEG in the critical care setting6-9, but neurological emergency patients can’t wait.

- Designed for outpatient & epilepsy evaluation
- Delays care due to wait times for EEG techs
- Limited after-hours availability
- Diverts resources from patients needing routine EEG studies
The lack of immediate, actionable brain monitoring at the bedside leaves clinicians facing a difficult decision: wait for an EEG and the neurology read, or treat based only on clinical suspicion.
Ceribell Point-of-Care EEG:
Built for Critical Care. Designed with Neurologists.
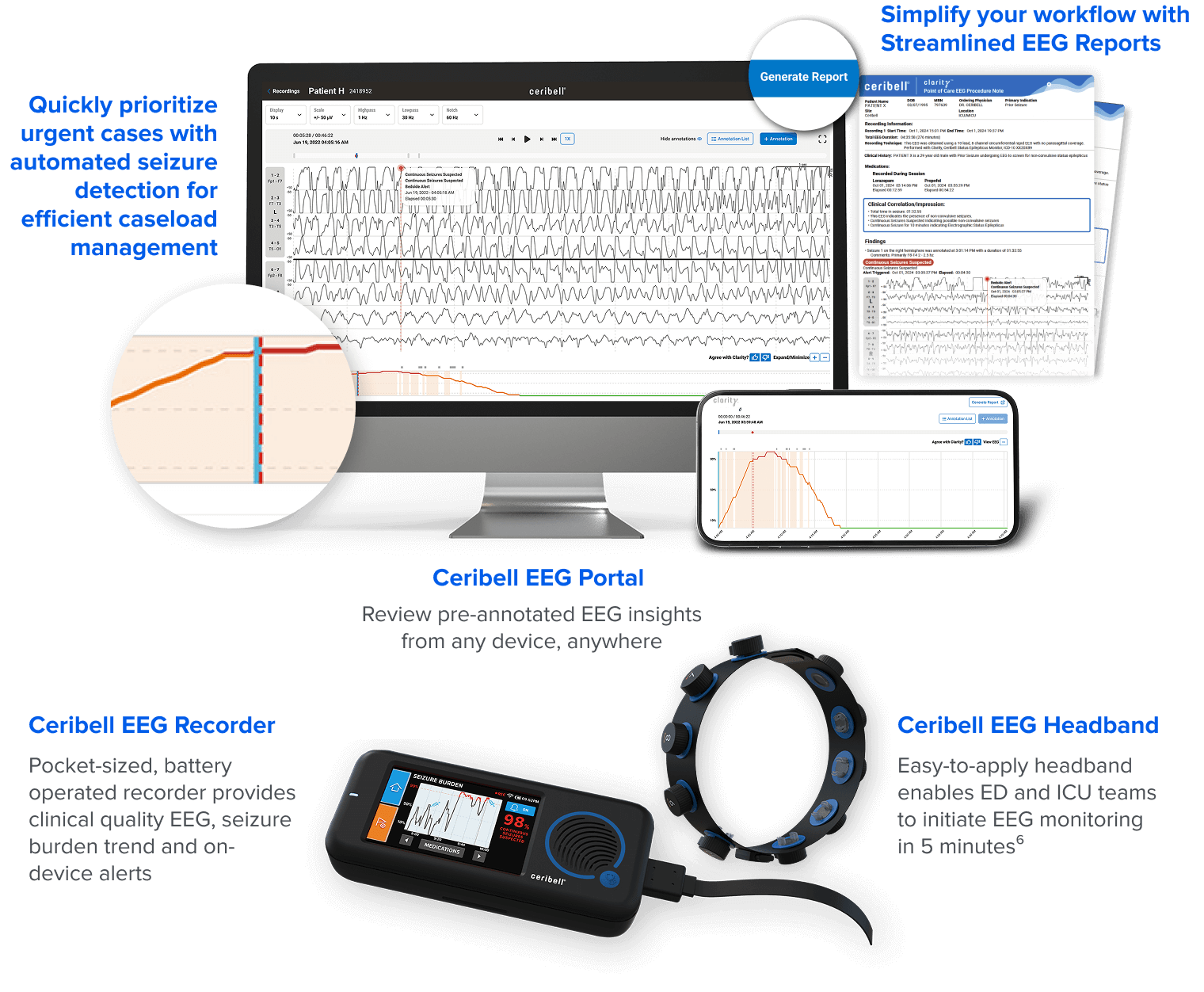

- Designed for emergency and critical care
- Real-time seizure burden monitoring
- Alerts for suspected status epilepticus based on NCS and ACNS definitions
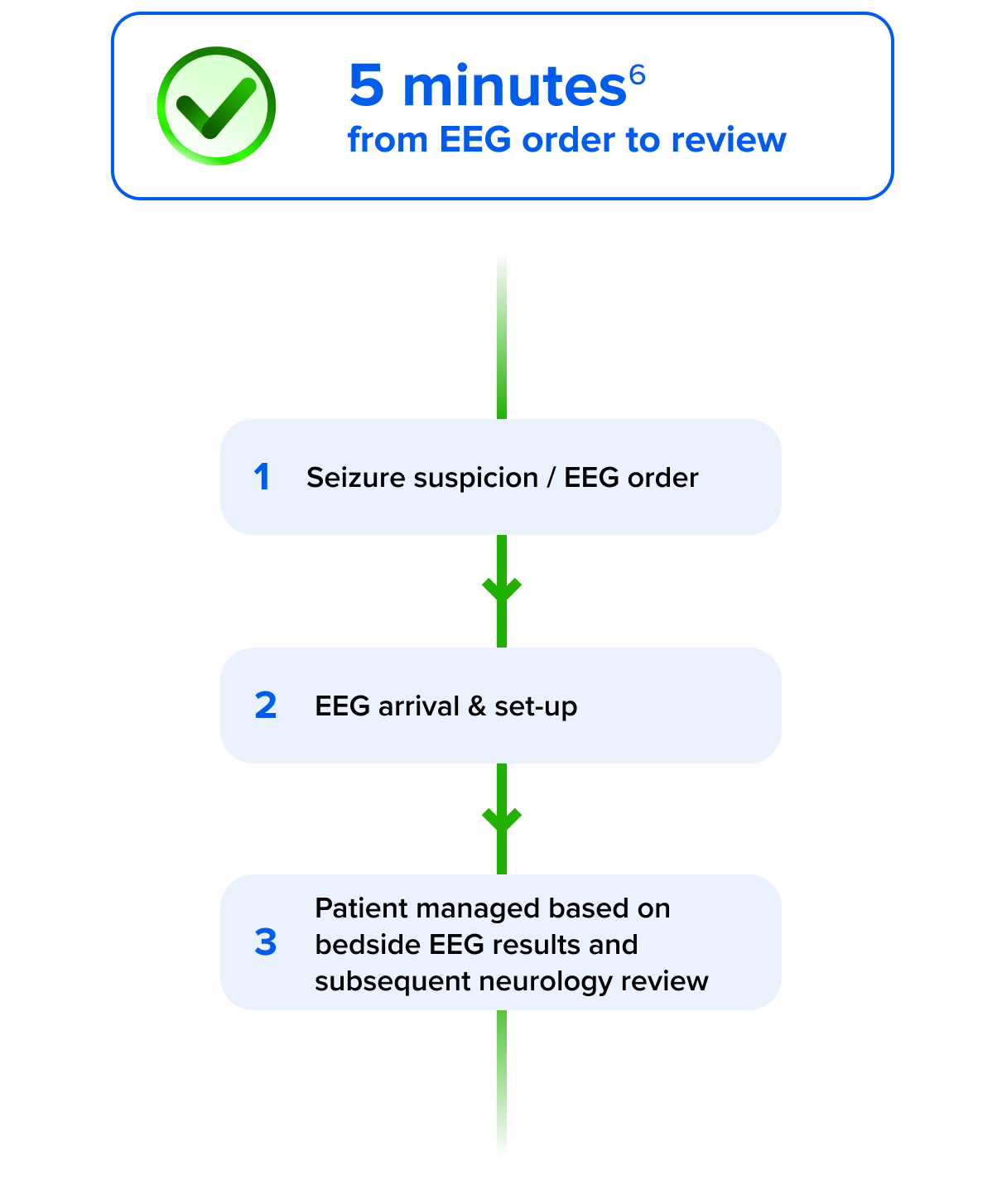
- Enables rapid bedside EEG in minutes6
- No EEG tech required for setup
- Supports fast triage and diagnosis
Ceribell POC EEG
Conventional EEG
Simplicity Matters When Time is Brain
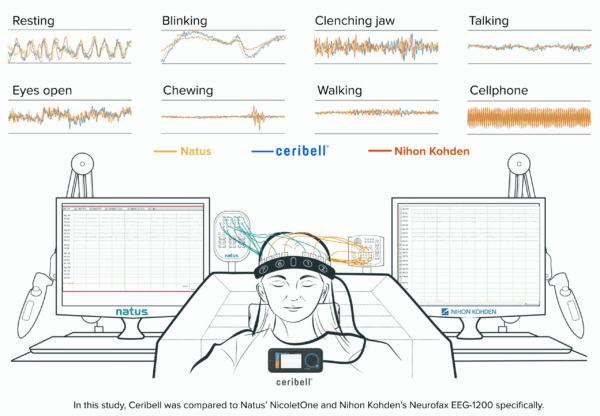
Ceribell offers equivalent signal quality to conventional EEG12
Ceribell has the optimal number of electrodes for seizure rule in and out
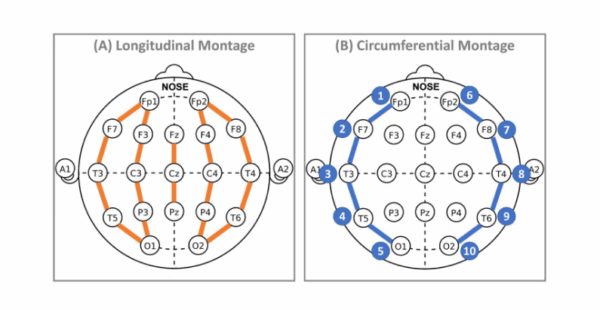
<1% of EEGs showed parasagittal seizures, all of which were visible in temporal channels and thus would be captured on Ceribell montage13
95% concordance diagnosis or ruling out of seizure activity between conventional and reduced montage like Ceribell14
In an emergency, you don’t need a full montage to know why a patient is aphasic.
No Added Hospital-Acquired Infections (HAIs) Risk with Ceribell
Disposable electrodes eliminate the need for electrode cleaning, disinfection or sterilization, greatly simplifying clinical workflows while delivering superior patient safety and institutional protection.
In addition to serious clinical implications, HAIs pose significant financial burdens on health systems, including:
Higher treatment cost15
Longer hospital stays15
Increased risk of mortality15
Regulatory penalties16
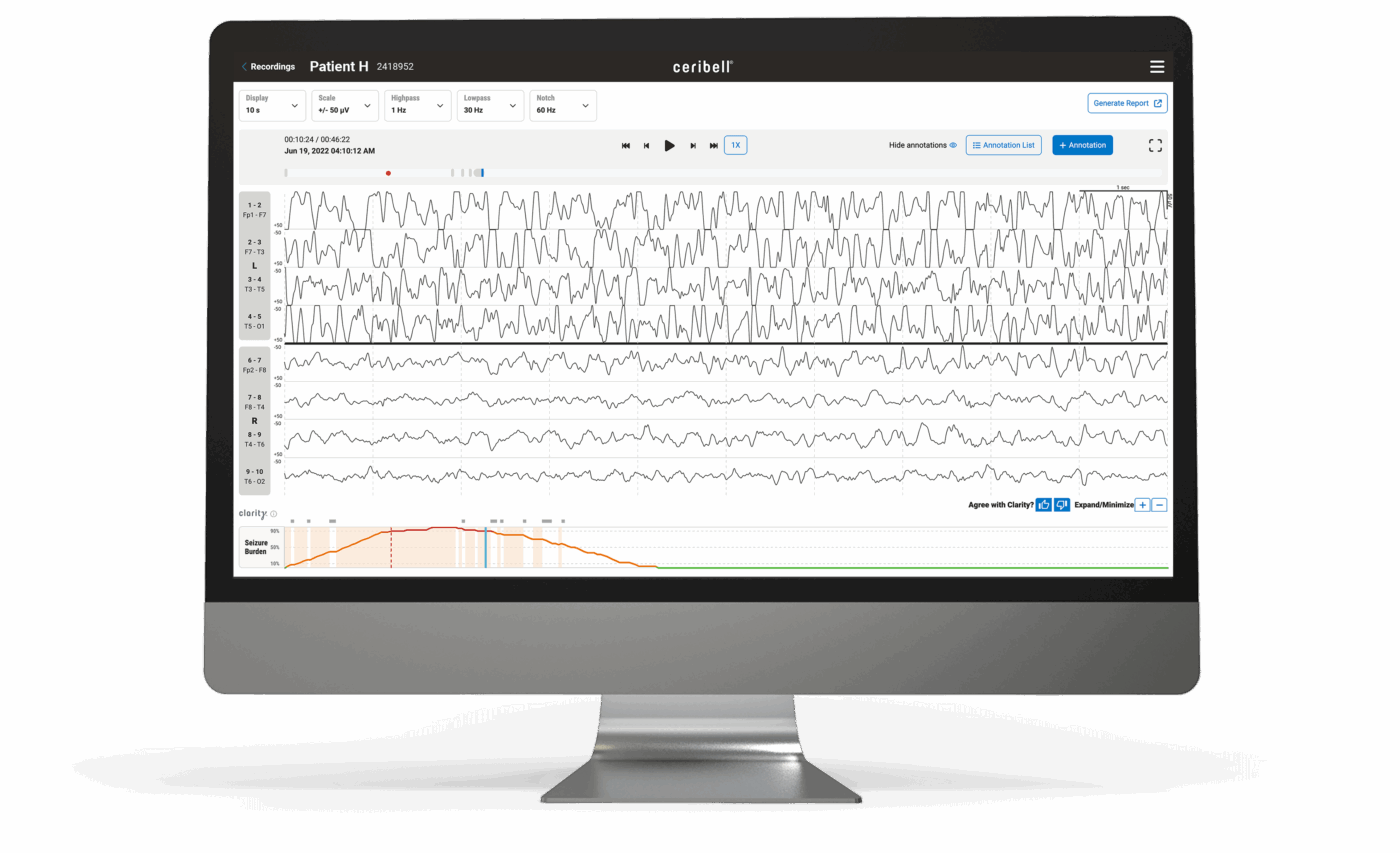
Performance You Can Trust
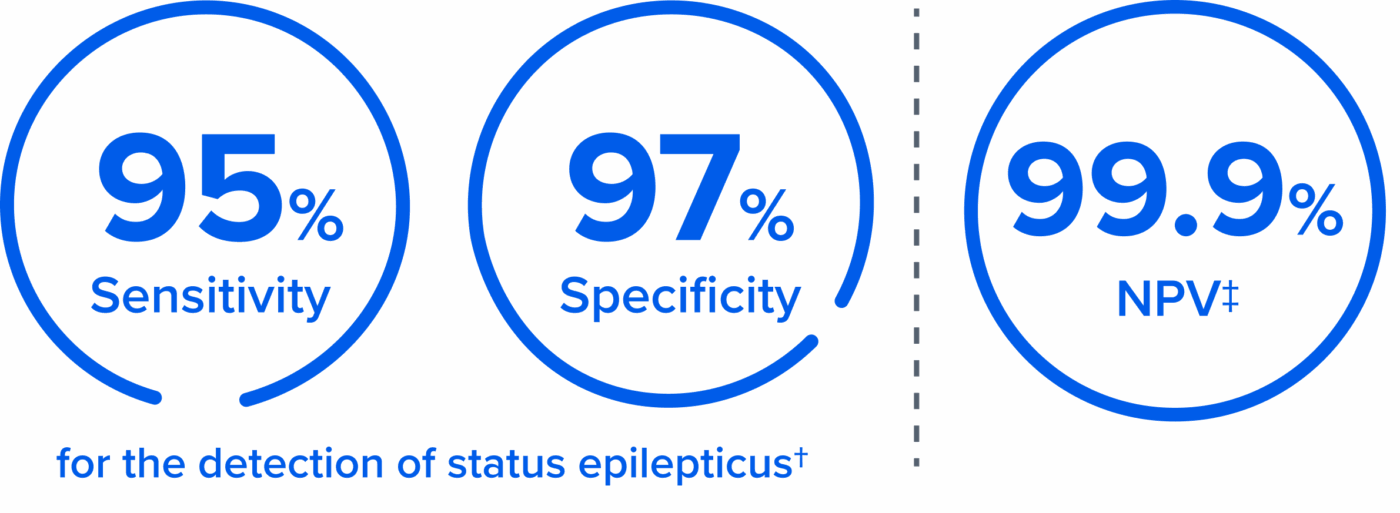
Clarity is validated to consistently alert for suspected status epilepticus and rule out seizure – on par with top epileptologists.17,18
The Ceribell Advantage
Intuitive, Secure Portal
Ceribell meets the highest cybersecurity standards and is one of only 51 companies to have FedRAMP High authorization from the VA.19

Native AI Integration
Clarity was developed using Ceribell hardware and using our continually expanding database of 1,000,000+ hours of expert-annotated EEG from ICU and ED patients.

Demonstrated Value
NTAP-eligible device offering up to $913.30 per eligible patient,11※ with proven length of stay and transfer reduction.20-23
The Evidence Leader
Ceribell is backed by 45 peer-reviewed publications,* including multi-center clinical studies like DECIDE6, SAFER-EEG20,24, and AccuRASE25.
Adopted by 600+ Hospitals* & Endorsed by Epileptology Leaders

Ready to Transform Your Neurology Practice?
Don’t let conventional EEG limitations compromise patient care. See how Ceribell can integrate seamlessly into your emergency and critical care workflows.




Resources
PAGE
Webinar
Ceribell Signal Quality Manuscript: Signals Recorded With Rapid Response EEG And Conventional EEG Systems
Read MoreIn The News