SAFER-EEG Trial
The Seizure Assessment Forecasting with Efficient Rapid-EEG (SAFER-EEG) trial is a retrospective study of 1074 adult patients from 4-top tier US academic hospitals who were monitored with EEG during their hospital stay from January 1, 2018 through June 20, 2022.

SAFER-EEG Study Subanalysis
Point-of-Care Artificial Intelligence Measure of Seizure Burden Associates With Clinical Outcome at Discharge1
Key Impact
Retrospectively estimated Clarity seizure burden was associated with increased disability and poorer functional outcomes at discharge, with increased effect size when including the output from the Insights Bar
Patients with ≥50% seizure burden had
Patients with ≥90% seizure burden had

Every additional hour of seizure associated with
Study findings show comparison against those with no findings per the relevant algorithm(s).
Study Overview

-
Secondary cohort analysis of 359 POC EEGs from 3 sites
-
Analyzed retrospectively by Clarity alone and combined with the portal-accessible algorithm (Insights Bar)
-
Poor outcome defined as a modified Rankin Scale score ≥ 4 at discharge
SAFER-EEG Study Subanalysis
Evaluating the Impact of Point-of-Care EEG on Length of Stay in the Intensive Care Unit2
Key Impact
Patients experienced a shorter median ICU length of stay and better neurological outcomes with Ceribell, compared to conventional EEG

shorter median ICU length of stay with Ceribell vs. conventional EEG

more patients from the Ceribell cohort had better neurological outcomes*

faster door-to-EEG time with the Ceribell System; 5.9 hours with Ceribell vs. 25.3 hours with conventional EEG
*Using modified Rankin Scale score (mRS) greater than or equal to 4 at discharge as an indicator of functional disability
Study Overview
-
3 sites had access to both Ceribell and 24/7 conventional EEG with technicians onsite or on-call.
-
283 ICU patients from the two cohorts were matched 1:1 with propensity scores to have equivalent age, admission scores, diagnosis group and seizure suspicion.
Author Research Overview
“Ceribell use is associated with shorter stays in the ICU and better functional outcomes, which are extremely impactful benefits to patients and their families.”
Masoom J. Desai, M.D., FACNS
Principal Investigator
Assistant Professor, Department of Neurology
University of New Mexico School of Medicine

SAFER-EEG Study Primary Analysis
Seizure Assessment and Forecasting With Efficient Rapid-EEG3
Key Impact
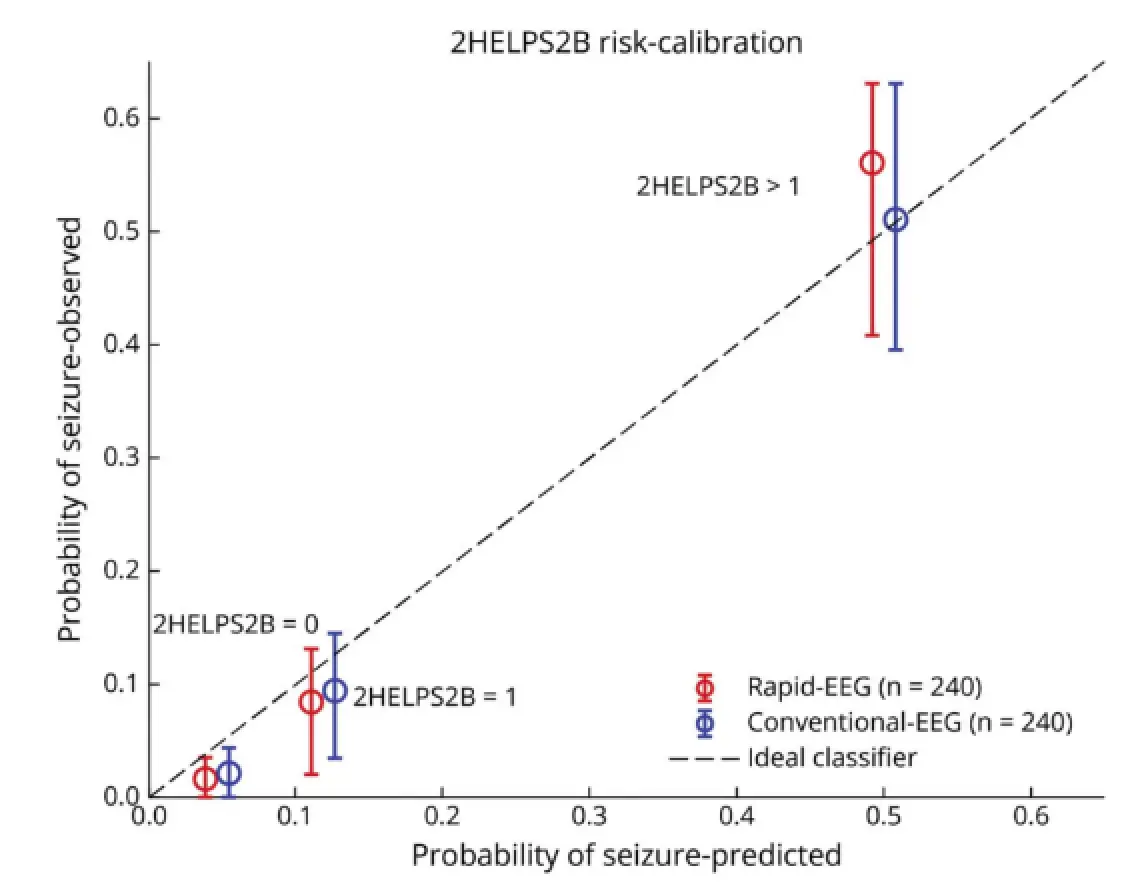
Performance of the 2HELPS2B score with Ceribell is comparable to conventional EEG for forecasting seizure risk in acutely ill patients
-
Comparable 72 hours in-hospital seizure risk forecasting with Ceribell vs. conventional EEG**
-
Similar false negative rate (0.021 with Ceribell vs. 0.016 with conventional EEG)
-
Similar seizure yield (9.1% with Ceribell vs. 12.9% with conventional EEG)
**As measured by 2HELPS2B score based on the first hour of EEG in matched cohorts
Study Overview
Results were published in Neurology, and demonstrate that Ceribell point-of-care EEG performs comparably to conventional EEG in forecasting seizure risk for acutely ill patients using the 2HELPS2B score.
- 240 Ceribell EEGs and 650 conventional EEGs were included and matched for confounders to evaluate the feasibility of using Ceribell EEG to assess future seizure risk at the hospital
- Estimated 2HELPS2B score for seizure-risk forecasting based on the 1st hour of EEG
Author Research Overview
“…the performance of the 2HELPS2B score on a rapid EEG is non-inferior to conventional EEG.”
Mariel Kalkach-Aparicio, MD, MBE
Physician Researcher and Neurology Resident
University of South Dakota

Resources
Clarity AI Study Manuscript: Monitoring the Burden of Seizures in Critical Care with a Novel Machine Learning Method
Read MoreIn The News
Clarity AI For 24/7 EEG Monitoring Alert – Manuscript Review With Dr. Josef Parvizi
Watch Our WebinarWebinar
Webinar