 Patient
Patient
64 y/o F w PMH of COPD (on home oxygen), pulmonary hypertension, heart failure w/ preserved ejection fraction, CKD 3, anemia, tobacco use, chronic UTIs, hydronephrosis, prolapsed bladder
 Timeline
Timeline
- Patient accompanied by husband & EMS to the ED due to AMS. Patient essentially unresponsive. Not following commands. GCS <8
- CT Head negative
- Blood cultures negative
- ABG w/ hypercapnea & respiratory acidosis. AKI.
- Intubated in ED and went into cardiac arrest
- Code x 14 minutes (compressions, defibrillation, amiodarone)
- Placed on a propofol infusion & midazolam 2mg given at 0800
- Transferred up to ICU, blood and urine cultures negative
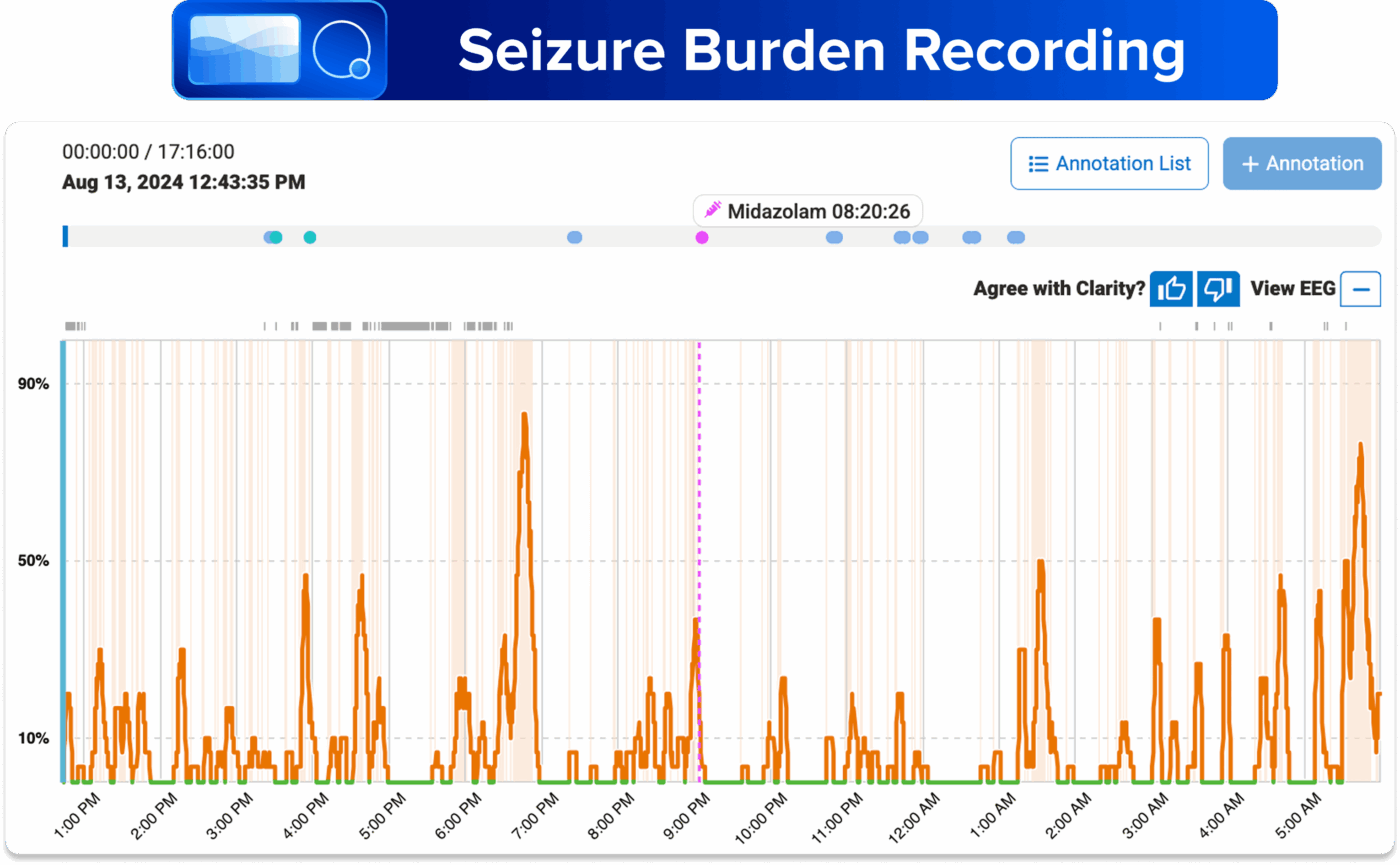
- Ceribell applied at 1243 due to concern for post-anoxic seizure in the ICU
- Max seizure burden reached 83.33% at 1830. Neuro confirmed EEG consistent with inter-ictal continuum
- Levetiracetam 2g and midazolam 2mg given at 1830 and 1900
- Midazolam given again at 2020
- Patient responsive and extubated the following day
Impact
- POC EEG provided prompt brain monitoring and real-time feedback on medication effectiveness.
- Neurology confirmed EEG improvement in response to treatment, coinciding with the patient becoming more alert and able to be extubated.
Case study is representative of real medical events.