
Clinical Data and Supporting Evidence
The Ceribell Point-of-Care EEG system has been clinically demonstrated to empower physicians to make faster, more accurate diagnostic decisions for informed treatment plans
Ceribell Impact and Accuracy
Ceribell Point-of-Care EEG was demonstrated to significantly improve clinical accuracy and confidence1
The DECIDE study was a prospective, multi-center observational study that evaluated the clinical impact of Point-of-Care EEG.
- Wait-time to Ceribell EEG was 5 Minutes compared to 4-hours with conventional EEG
- Diagnostic accuracy with Ceribell EEG was 90% versus 65% Using Clinical Judgement Alone
- Diagnostic confidence was 86% with Ceribell versus 40% Using Clinical Judgement Alone
Ceribell Utility in Emergency Care
Ceribell use in the ED has the potential to positively impact the clinical management of suspected nonconvulsive seizures2
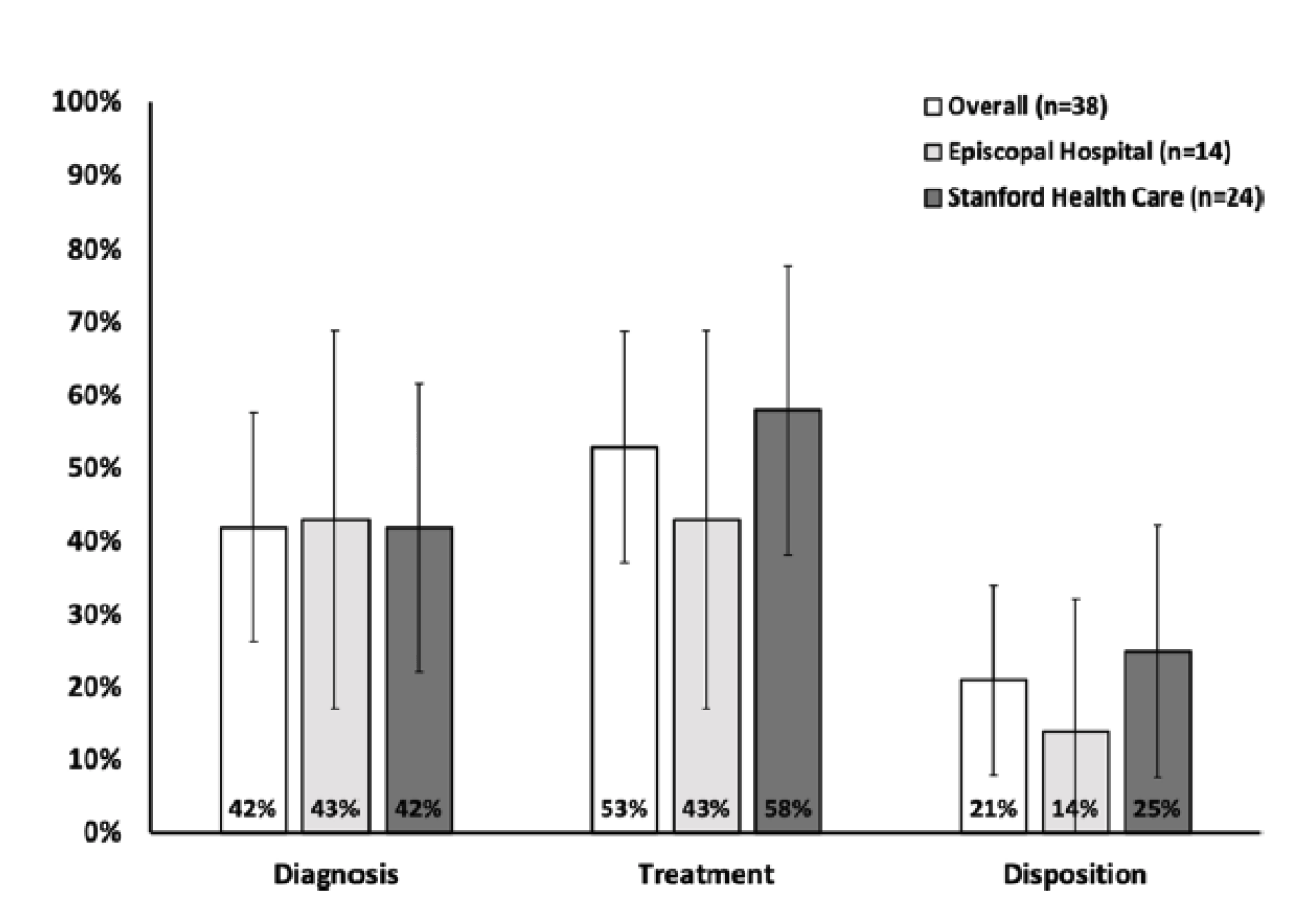
This prospective study conducted at two ED sites evaluated rapid EEG impact on seizure management when used by emergency physicians.
- Ceribell changed clinical management for 53% of patients
- Ceribell expedited treatment in 21% of patients
- ED physicians identified seizures with 100% sensitivity and 92% specificity when using Brain Stethoscope
Ceribell Utility in Intensive Care
Ceribell use in ICU allowed rapid triage and has the potential to improve clinical decision making and prevent overtreatment3,4
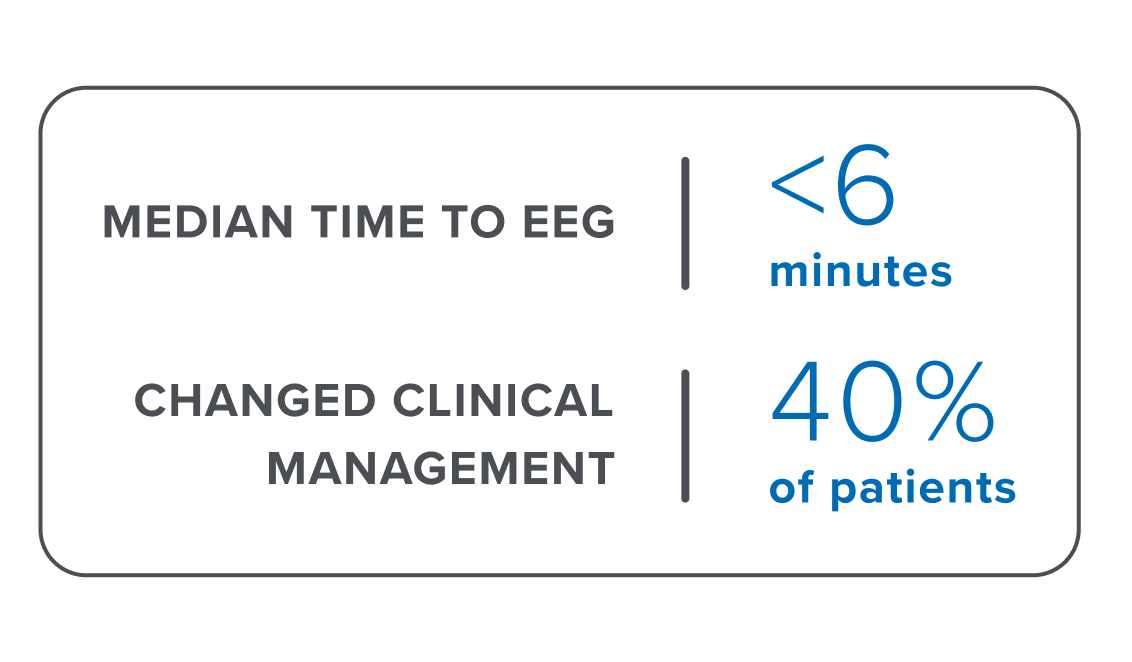
Prospective studies conducted at two ICU sites evaluated rapid EEG impact on clinical decision-making when used to triage seizure in the ICU.
- Set-up time for Ceribell was within minutes at both sites (5-6min)
- Use of Ceribell changed treatment decisions in 40% of cases at both sites
- These results were further confirmed by results from the DECIDE multi-center study
Clarity
Ceribell with Clarity provides 24/7 EEG monitoring with consistently high performance for assessment of suspected status epilepticus5
The NEW Clarity study was a retrospective, 11-center study with a larger sample size that evaluated the performance of Clarity to measure the burden of seizure activity and generate bedside alerts for possible status epilepticus.
- 95% Sensitivity for alerting to non-convulsive status epilepticus
- 99.8% negative predictive value for ruling out seizure
Signal Quality
Ceribell electrode signal quality was equivalent to conventional EEG6
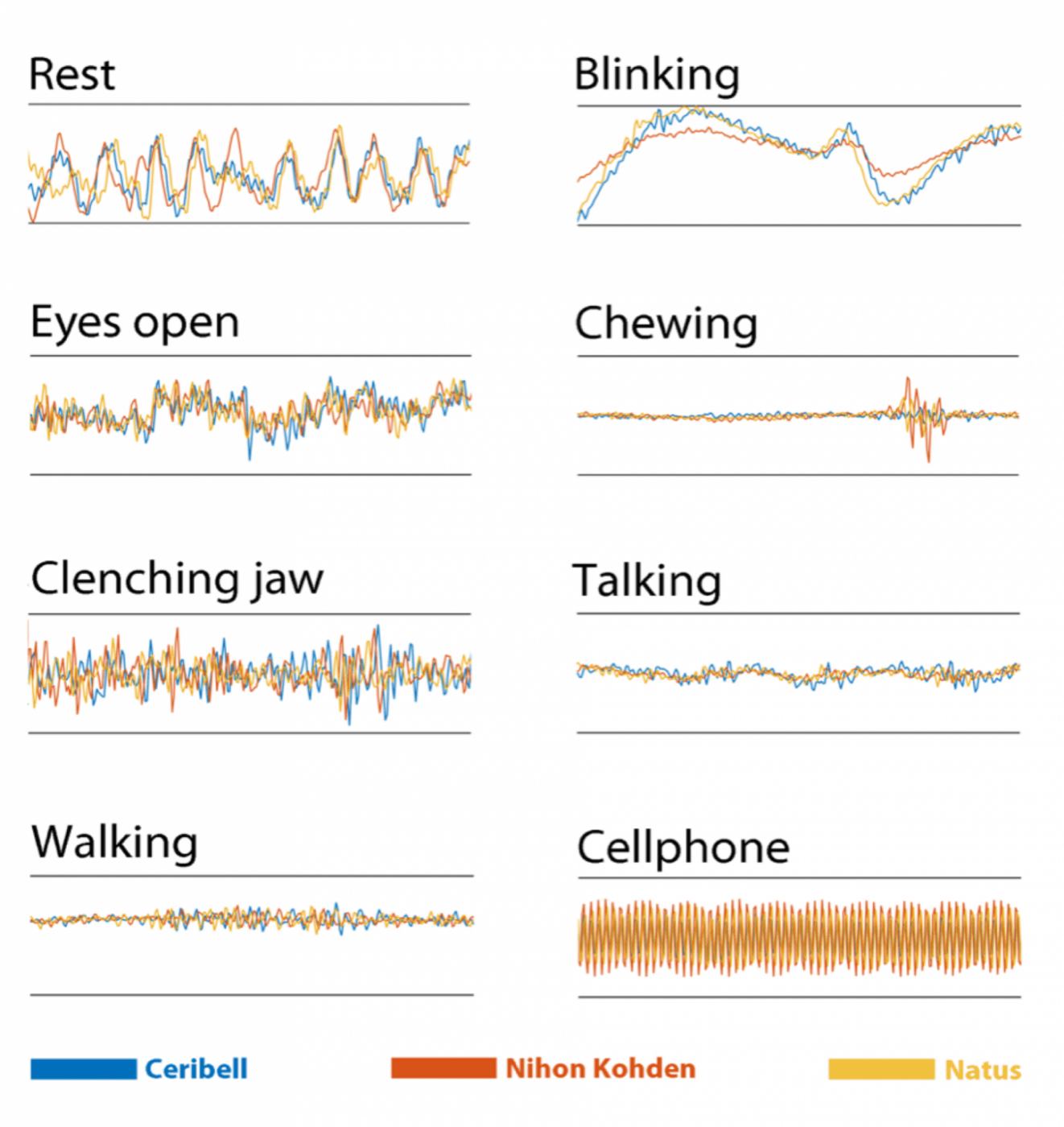
This study assessed signal quality of the Ceribell EEG system compared to that of two conventional EEG systems to confirm the Ceribell signal quality performance was equivalent to gold standard conventional EEG. Ceribell electrodes were placed side-by-side on the same patient with traditional EEG system electrodes and simultaneous recordings were then compared.
- The two EEG results showed equivalent signal quality and durability (see overlaid signal).
Montage
EEG recordings using a circumferential 10-electrode montage meet the gold standard for seizure detection7
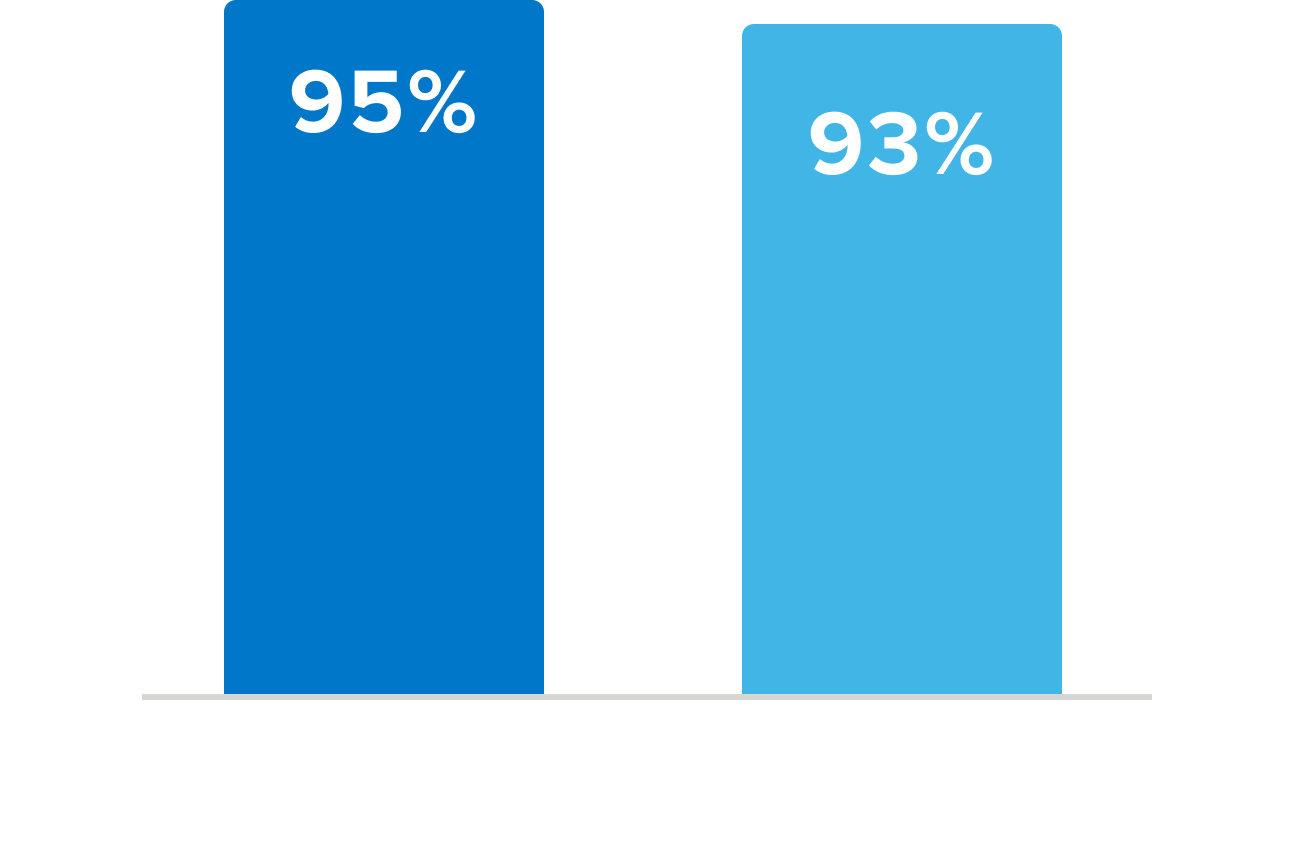
This study assessed whether reduced montage EEG (rm-EEG) systems, like that used by Ceribell, meet the gold standard full-montage EEG (fm-EEG) for detection of seizures. In the case of discordant diagnoses, it further sought to determine whether the difference was due to electrode reduction or to asymmetric access to ancillary information. 212 fm-EEGs were reviewed with access to ancillary information. The same EEGs were converted to rm-EEG (10 electrodes) and different neurologists read them with no ancillary information. EEGs with discordant readings between the two groups were then reviewed again with no access to ancillary information.
- The rm-EEG resulted in high diagnostic concordance (95%) with fm-EEG and high agreement between EEG-readers (93%) when ancillary information was equal
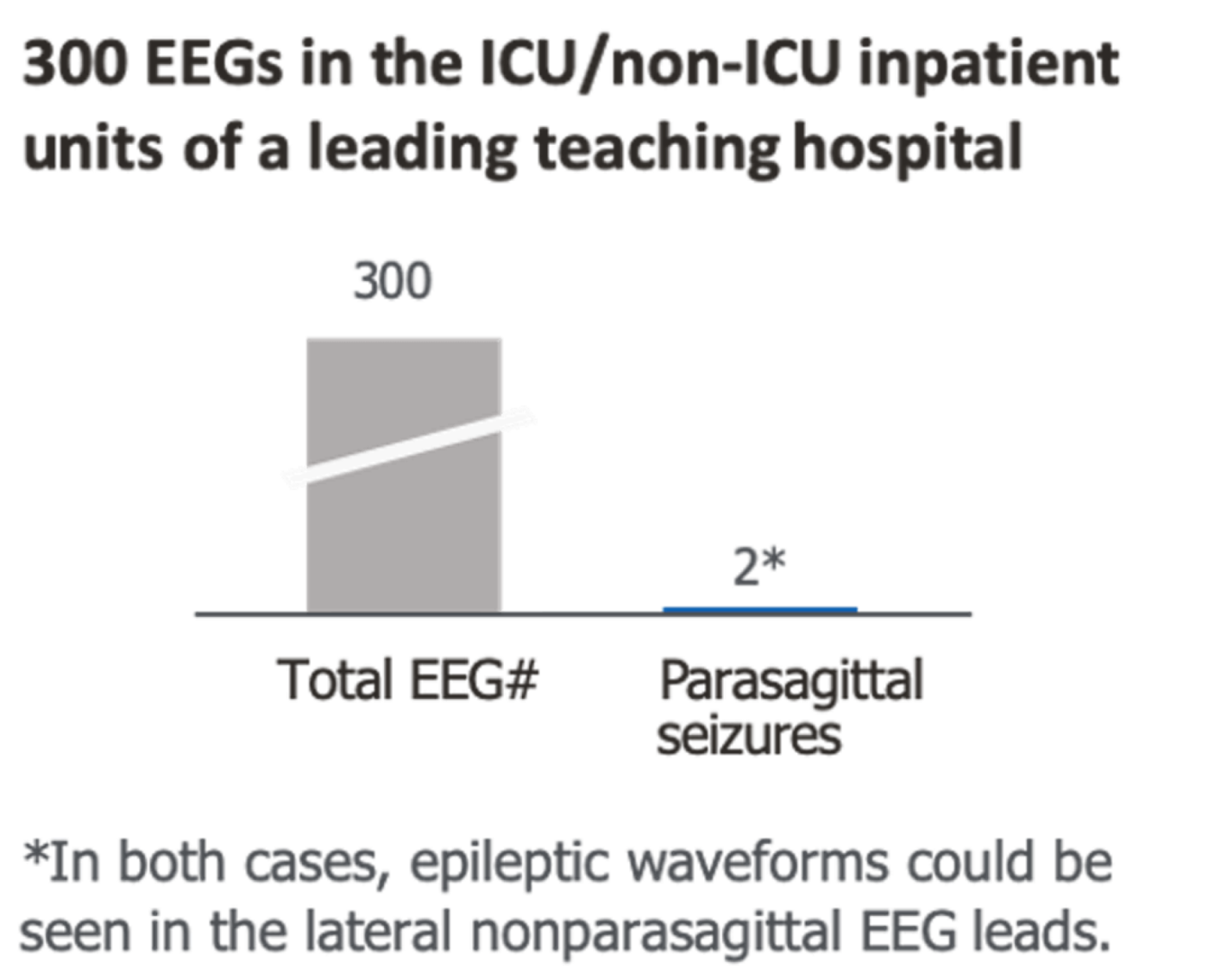
Focal parasagittal and midline epileptiform activity is rare and can be seen in temporal leads8
A retrospective review of 300 EEGs and >169k cases reported in literature confirms that only 0.7% of EEGs show focal parasagittal/midline seizures.
- The prevalence of midline or parasagittal abnormalities was only 0.71% (1,211 of 169,510) in the 16 published works
- In a cohort of 300 patients, 17 were found to have seizure activity, and of these, only two were focal midline or parasagittal seizures and both could be detected in lateral chains of the EEG
Health Economics
Ceribell Point-of-Care EEG alters the treatment course for patients with suspected seizures and will result in cost savings per patient9
This study built a two-armed cost–benefit model comparing rapid EEG with clinical suspicion alone to examine the effect of Ceribell on hospital costs.
- Ceribell led to reduction in the hospital LOS by 1.2 days (6.1 vs. 7.4 days) and ICU LOS by 0.4 days (1.5 vs. 1.9 days)
- Rapid EEG savings was $5,633 per use case (95% PI: $4,649 to $6,617)
- Cost-savings were demonstrated in 75% of replications
- 64% of variance in total costs was attributable to LOS for persons incorrectly diagnosed with seizures


Resources
DECIDE Study Assessing The Impact of Ceribell EEG – Manuscript Review With Dr. Paul Vespa
Watch Our WebinarWebinar
In The News
In The News